 es
es en
en fr
fr it
it ru
ru ar
ar zh-hans
zh-hans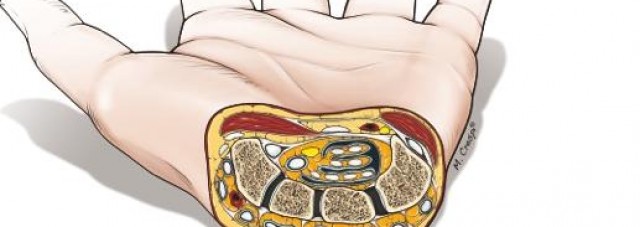
Ci-dessous vous pouvez lire une traduction de traducteur humain en anglais. Vous avez également accès à l’original espagnol en cliquant sur le drapeau dans le coin supérieur droit. Ce lien vous donne accès à une version de traduction automatique de Google en français: http://bit.ly/2L1Rph7
The nocturnal pains that prevent falling asleep, the constant tingling and the hands that feel numb, the loss of sensitivity and manual ability, turn the carpal tunnel syndrome into a real daily curse for those who suffer it.
A desperating situation which can make the patient susceptible to put their trust in ‘new surgical routes’, whose risks far outweigh some more than doubtful possible benefits.
Dr. Francisco del Piñal defends the clinical results of the current minimally invasive technique, and warns against what he calls “siren songs” of the alleged solutions by endoscopy or laser, which “prioritize commercial interests over those of people”.
Dr., what is the current status of the surgical solution to carpal tunnel conditions?
The surgical techniques of the carpal tunnel have evolved a lot during the last two decades. In the past, this intervention involved general anesthesia, an incision of about ten centimeters and the use of plaster. Today, the ‘cut’ is only two centimeters, the anesthesia is local and we talk about outpatient surgery; that is, the patient returns home at the conclusion of the operation, with a postoperative process, in addition, that does not imply immobilization.
However, despite these advances, we must be cautious about the promises of solutions through percutaneous surgery or laser. There are numerous commercial interests, which are -unfortunately- above those of the patient.
Do you doubt the effectiveness of this type of techniques?
I do. In fact, there is no surgical laser technique that can be applied to carpal tunnel problems. Sometimes, it is confused, deliberately, with endoscopy. And the point is that’s ‘nice’ to present the patient who is operated an incision of a centimeter and a half.

Don’t they offer benefits to the patient?
No, none. The technique that we use, for example, involves similar incisions, but it allows us to see the superficial and deep nerves of the intervened area; the most vulnerable part and exposed to irreversible consequences in this operation.
Neither are recovery times reduced, not even the immediate post-surgery discomfort. After three months, the results are identical so is not worth it, in any way, to take the risks that you pointed out.
It doesn’t offer aesthetic benefits in the final appearance of the area either, and, if that were not enough, it needs axillary regional anesthesia.
Endoscopy, in this case, implies a stronger anesthetic need, I guess (…)
So is. There are many factors, as you see. Plainly, we talk about benefits that are purely imaginary.
Risks and sequels?
Unfortunately, ‘forced’ procedures by endoscopy can damage nerves, tendons and even arteries. All the elements of the carpal tunnel are very compressed, and the risk techniques we are talking about involve inserting a needle, a scalpel and an endoscope, in whose end – in this case – a blade is placed, which is the one that must ‘cut’ the zone from within.
I have operated on patients who had suffered sections, that is cuts, of larger nerves; a sequel that we can hardly ‘mend’ and that causes irrecoverable functional limitations to the affected people, with pain for life in some cases.
We must bear in mind that the operations associated with carpal tunnel syndrome are more common in people in the second half of their adult life, and that they already accumulate a natural deterioration in the affected area; what makes the picture worse.
What’s the prevalence of these types of sequels?
Carpal tunnel syndrome makes it difficult for the patient to perform the most usual daily tasks, a problem for which there is a solution outside of techniques risky and of doubtful clinical benefit.

We speak, statistically, of 1 case out of every 100 with serious sequels. However, in a type of operation so usual this supposes an unacceptable number of people affected; especially when we have technical alternatives that eliminate this risk, and offer the same or better medical results.
My recommendation for patients is to be cautious about the ‘siren songs’ that promise surgery by laser or endoscopy, or speak of percutaneous incisions for the carpal tunnel.
From what you say, Dr., I infer that the technique that you and your team use minimizes the risks (…).
True. We use magnifiers and surgical microscopes. With retraction, technique and care, we open the carpal tunnel without endangering any of its vasculonerval structures. As I was saying, we intervene in a minimally invasive way, and the patient returns home after completing the operation; without having undergone total or locoregional anesthesia and without suffering limited hand mobility.
Being straightforward, this technique is the best, without discussion. The use of lasers is a commercial invention, without further ado, it does not exist. Let me insist, endoscopy is great in other clinical situations, but not in the case of carpal tunnel syndrome. It does not provide a single demonstrable advantage that compensates for its risks.
To be even clearer and not offer doubts, if I myself needed to have an operation in the carpal tunnel, I would never resort to endoscopy.
Related content: