 es
es en
en fr
fr it
it ru
ru ar
ar zh-hans
zh-hans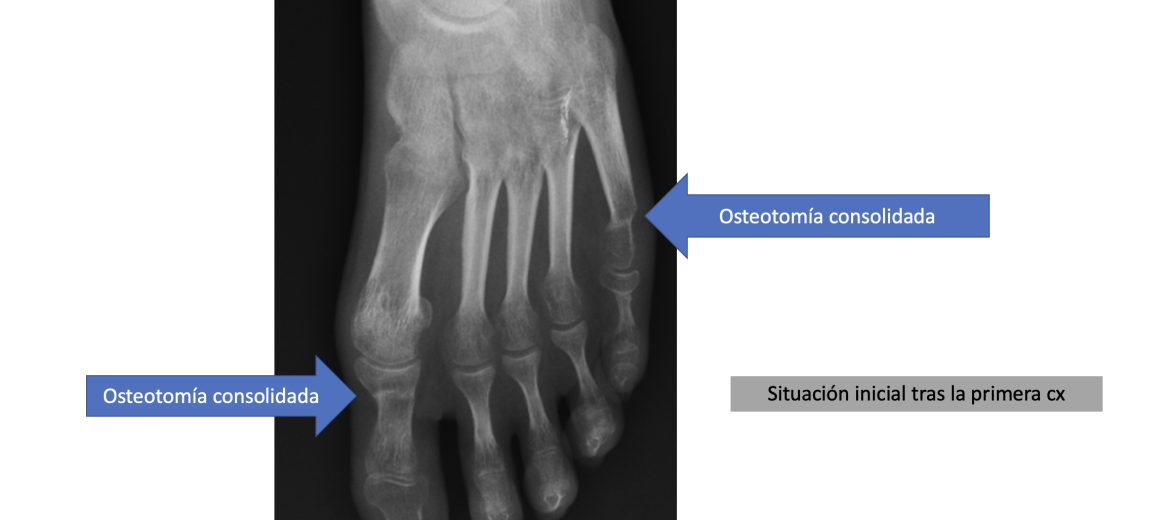
This involves a 23-year-old patient presenting with chronic pain on the outer edge of the left foot after being operated on for an acquired deformity years ago. She needs crutches to walk as the pain upon bearing weight is intolerable, interfering with all her activities.
Custom osteotomies are an optimal resource for correcting atypical bone deformities, whether congenital or acquired in the context of an intervention.
An osteotomy involves breaking a bone with the intention of repositioning it in a specific way to relieve a condition. The fact that an osteotomy is consolidated, meaning the fracture has healed, does not necessarily mean that the desired goal has been achieved. The bone fragments may have fused but not in the ideal position planned beforehand, partially correcting the initial problem or even aggravating it or generating a different one than the original.
This is a 23-year-old patient seeking help for chronic pain on the outer edge of the left foot after being operated on for an acquired deformity two years ago. She needs two crutches to walk as the pain upon bearing weight is intolerable, interfering with all her activities.
Specifically, she had undergone osteotomies to correct interphalangeal hallux valgus, meaning the first toe deviated outward, as well as varus of the fifth toe, deviated towards the opposite side, using a percutaneous technique.
During the postoperative period, the painful symptoms persisted for more than 6 months, and clinically the diagnosis of Südeck’s disease was determined, leading to referral to the Pain Unit after ruling out any surgical solution.
A CT scan was performed, revealing that while the osteotomy was consolidated, it had been performed in a plantarized position, meaning with the head turned towards the ground at a greater angle compared to the head of the first metatarsal.
The objectives were to achieve a pain-free foot with weight-bearing capacity to regain function without the need for crutches. Correct the deformity in plantarization of the head of the fifth metatarsal, as well as the contracture in flexion of the proximal interphalangeal joint. Perform a custom osteotomy to elevate, without further shortening, the head of the fifth metatarsal, thus relieving the load it receives and transferring it to the rest of the toes. Finally, carry out a fibrous joint arthroplasty procedure, eliminating the flexion of the toe that causes abnormal contact with the ground, leaving it straight.
The results are that at 3 months, the osteotomy is consolidated in the new ideal position, and the patient has no pain with weight-bearing, allowing her to walk without crutches in normal footwear. The patient has been able to regain her normal life, transitioning from being dependent on crutches without support to walking normally.